If you have any questions about genome editing, email our research team research@musculardystrophyuk.org.
Genome editing
Skip to section
What is genome editing?
Genome editing is a technique that allows scientists to change the DNA, the molecule that contains the genetic code of cells or whole organisms. It can be used to add, remove or replace part of the DNA. If changes are made within a gene, the technique is sometimes referred to as gene editing.
There are several genome editing systems that scientists can use. Although they differ in cost, efficiency and accuracy, they all share a common component – an enzyme (a protein that can initiate or speed up biological processes) called a ‘nuclease’. This enzyme cuts the DNA at a specific location, acting like a pair of molecular scissors. The cell then re-joins the DNA through its own natural repair processes.
The most commonly used genome editing system is CRISPR/Cas9, which was originally discovered in bacteria as a natural defence against viruses. You can think of it as ‘a guided missile, targeting precise sites’ in the genome. The Cas9 nuclease acts like the missile, while the CRISPR part is the guide system, telling Cas9 where to hit.
What is genome editing used for?
Currently, it’s mostly used in research. But given that it has the potential to alter any DNA sequence – in bacteria, plants, animals or humans – it could also be used in:
- medicine, to treat or prevent a genetic disease
- agriculture, to protect crops from drought or disease
- environment, to control insect populations that transmit diseases
- industry, for biofuel or chemical production.
In research, scientists also use genome editing to understand what genes do and how they contribute to the way we are. For example, scientists may try to model a human disease in cells or animals by deleting or editing a gene thought to contribute to the disease. If these models do mimic the disease, they could then be used to test new therapies.
What’s the difference between gene therapy and genome editing?
Broadly speaking, gene therapy is the use of genetic material to treat a disease. Depending on the disease, this could involve:
- introducing new genes in order to boost production of a desired protein
- correcting changed (mutated) genes, so that they are functional again
- silencing genes that are causing problems.
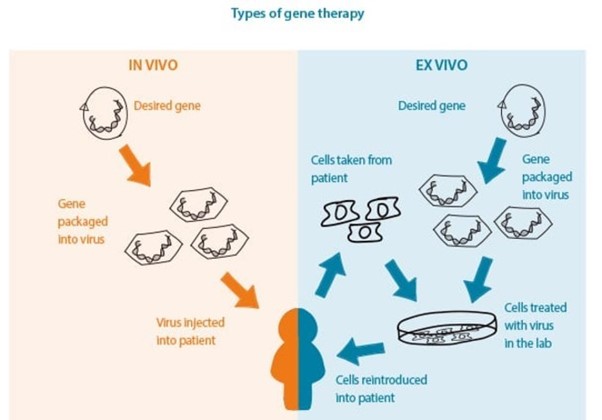
Genome editing is a form of gene therapy when it’s used to treat a disease. This sort of therapy can be injected directly into a patient (in vivo), or into cells from a patient (ex vivo), which are then transplanted back into the patient (see below). Researchers around the world are investigating the potential of genome editing as a treatment for muscle wasting conditions.
What are the challenges with genome editing?
Although the molecular scissors are targeted to a specific point in the genome, they can sometimes cut in the wrong place – this is known as an off-target effect. Off-target effects could be dangerous if they disrupt healthy genes or important regulatory DNA. Although there has been a lot of research to refine genome editing techniques, we still don’t fully understand the risk of off-target effects. Scientists need to address this before we can use genome editing in the clinic.
Another challenge is how to get the genome editing system into the cells of the body. It can’t travel around in the blood like other drugs can, as its consisting parts are too large. It needs to be packaged up into something called a ‘vector’, which can enter cells more easily. Several vectors are being investigated, including different types of viruses and tiny molecules called nanoparticles.
Why is genome editing controversial?
In addition to questions about its safety, there are some ethical concerns about genome editing. If genome editing were used to change the DNA of a human embryo, these changes would be hereditary, in other words they would be passed down to that person’s children and to future generations. Some people have moral and religious objections to manipulating embryos in this way. Currently, researchers in the UK need to have a licence from the Human Fertilisation and Embryology Authority to carry out genome editing in human embryos. However, it is illegal to keep the embryos beyond 14 days after fertilisation, and they cannot be transferred into a person.
A survey by Royal Society showed that the majority of the UK public supported the use of genome editing to treat incurable diseases. However, there is a concern that this could lead us down a ‘slippery slope’ to using it for cosmetic reasons or enhancing abilities. It’s important that scientists, clinicians, regulators, policymakers, patients and the general public continue to discuss these issues and shape the UK’s policy and regulation of genome editing.
What’s the potential of genome editing for muscle wasting conditions?
As many muscle wasting conditions are genetic, in other words they are caused by a change in a gene, they could potentially be treated with genome editing. Researchers around the world are looking into this for several muscle wasting conditions, including Duchenne muscular dystrophy, congenital muscular dystrophy, facioscapulohumeral muscular dystrophy, myotonic dystrophy, limb girdle muscular dystrophy and mitochondrial disease.
A previous study by researchers in the UK and USA showed that a CRISPR/Cas9 therapy could correct the dystrophin gene in a model of Duchenne muscular dystrophy. This boosted dystrophin production in the animal’s muscles, heart and diaphragm. The muscles also appeared healthier, but we don’t know how functional they were as the researchers didn’t assess this. While these results are promising, the study was too small and too short to know whether the CRISPR/Cas9 therapy was safe and effective. It’s important that larger, longer-term studies are carried out.
When will it be available?
Although there have been some promising advances recently, there’s still a lot we don’t know about the safety of genome editing. A lot more research is needed before the technique can be trialled in people with muscle wasting conditions. It’s difficult to estimate how long this might take, but it’s hoped that we can learn from advances in research into other conditions along the way. There are currently genome editing therapies in early clinical trials for several conditions, including beta-thalassemia, sickle cell disease and some types of cancer.
If you have any questions about genome editing, email our research team research@musculardystrophyuk.org.
Questions about genome editing
Current research projects
We fund pioneering research for better treatments to improve people’s lives today, and to transform those of future generations.